There must be a special sort of vulnerability that comes from an economist staking her reputation on market projections. Or from Stephen A. Smith when he stares right into ESPN cameras to belittle the Cowboys before and after every game (but, by God, he’s been right for 29 years).
I’ve never been brave enough to share my predictions publicly. Recently, though, I feel more assured of my judgments. I may be getting smarter, or more reckless, or perhaps a man just loses all sense of ego when his five- and three-year-olds beat him into submission.
Regardless of why, I’ve decided to dip my toes into forecasting by reacting to others’ predictions. Nikhil Krishnan, founder of Out of Pocket Health—and a treasured source of healthtech comic relief—recently published two blogs: one with his own predictions, and another featuring some of his readers’ predictions. And, though I could probably use a hair transplant from Turkey, I’m going to skip Nikhil’s take on medical tourism and dive into a couple of healthcare data-oriented predictions in his posts.
Data standards rendered obsolete?
Original prediction:
We won’t see accelerated adoption of interoperability standards (e.g., HL7®, HL7® Fast Healthcare Interoperability Resources or FHIR®). The combination of evolving data lakehouse architectures and powerful generative AI unlock unprecedented value in loosely structured and unstructured data. Increasingly, machines are much less discriminating between a finely structured FHIR document and a poorly scanned PDF—and the latter may be richer than the former. Nick Stepro, Chief Product Officer at Arcadia
I can agree with this, but only when it comes to a very small subset of healthcare data and AI users. The argument makes sense in the abstract or hypothetical use of large swaths of healthcare data for ML training and insight.
But outside of cutting-edge data scientist applications, this prediction makes less sense. In my experience, a newly innovative health system isn’t anywhere close to being prepared to leverage cloud tooling at this level of complexity. In fact, most health systems (and their EHRs) have to spend more time ensuring that their technology complies with basic regulatory requirements, which is what actually pushes the cart in terms of technology adoption. And, nowadays, those regulatory requirements are heavy-handed with FHIR interoperability.
It seems too early to suggest that FHIR or HL7v2 are going to start dying on the vine thanks to lakehouses or AI, when the whole purpose of these standards is not to offer a fancy database schema (or to contradict your database schema). Rather, these languages were made to convey data accurately, and perhaps inefficiently, to reduce administrative burden and enhance basic transitions of care between systems that have completely different schemas and simply need a common language.
With the push for interoperability, I expect standards will survive for a long, long time. Hell, HL7v2 is older than me and has several successors trying to make it obsolete, but guess what, baby? We’re only 30, flirty, and thriving *hair toss.*
Providers want more of the non-services pie
Summary of original prediction:
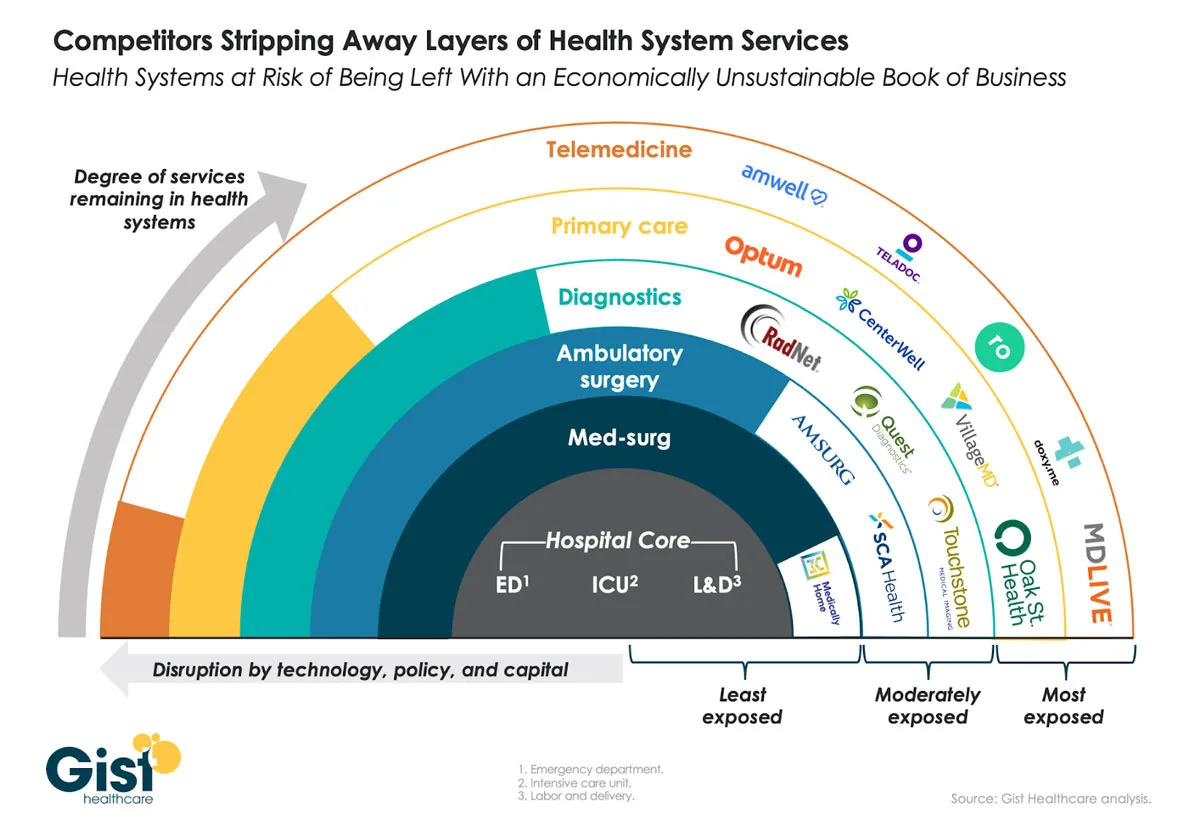
Major health systems are seeing new, tech-forward competition converge on what used to be unexposed revenue streams (e.g. telemedicine, primary care, diagnostics, etc.). In an attempt to box out this competition and further entrench themselves in markets where there is a barrier to entry, Nikhil suggests health systems may offer more provider health plans and commercialize in-house IP, technology, and data.
I love this one. And I’m not so sure it’s a risky take. In fact, it’s not just providers who want more of the pie, but payers as well (this Economist article talks about how the law incentivizes payers to verticalize their business). Recently, I spoke with a major provider’s Chief Data Officer, who loved the following Gist Healthcare diagram (which I totally ripped from Nikhil’s article). I owe Nikhil a beer for teeing this up for my talking points.
Unsurprisingly, organizations that are big enough are diversifying their offerings or acquiring companies towards whatever end of the healthcare spectrum they don’t already dominate. Verticalizing and diversifying an organization’s reach in services/insurance not only adds to these groups’ revenue streams, but it also provides them an opportunity to collect and recycle data to which they otherwise would not have had access. And, as Nikhil suggested, they can try to commercialize the data in a number of ways, especially if they are hopping on the healthcare data train with hyperscalers like Databricks, Google, Microsoft, and Amazon.

Inquiries into utilization management
Summary of original prediction:
Utilization management and prior authorization workflows are so broken that some payers are being caught flat-footed when investigative journalism questions why good people cannot get coverage for reasonable care. Capitol Hill should have an easy line of sight into criticizing the processes between payers and providers and proposing a new regulatory framework that normalizes and streamlines claims and claims denial processes in the long term.
Nikhil is already pretty much right on this one, thanks to the Final Rule issued on January 17th. Regardless of whether you are a payer, provider, payvider, or a patient, you probably hate Prior Authorization. Fortunately, I don’t have too much real-world experience with waiting for medical treatment while other people fax my records back and forth, but my daughter did swallow a galvanized bolt one time and her pediatrician is still documenting on paper (you have no idea how badly I want to lecture those adults). The resulting diagnostic image referrals might as well have been sent back to 1979 so Judy Faulkner could handle them from a basement in Madison, Wisconsin.
Anyway, back to utilization management. I think it’s fair to say that as payers and providers modernize, consolidate (see previous prediction), and buy expensive software, they will also be interested in at least plotting a vision to interoperate for the sake of more decisive utilization management. Plus, other data interoperability efforts like TEFCA (which admittedly has about the same number of users as Omegle) and Carequality are making it easier for federated organizations to exchange clinical summary information. Although this doesn’t aid payers just yet, it will in the future as approved use cases expand. Just ask the On-Ramp Overlord, Brendan Keeler.

Parting thoughts
With 2024 well underway, the only surprise so far has been that no one has acquired a major Medicare Advantage payer. We’re bound to see exciting but safe innovations stemming from Generative AI. Giants of the industry will continue to prepare themselves for a perpetual M&A cycle by creating “system-agnostic” technology and databases, and mostly I’d guess that a requirement for data acquisition and data engineering will precede many innovations in healthcare software, which is okay!
If you have comments, questions, or objections to this article, reach out to me at [email protected]. I’m happy to learn from other industry perspectives.